

An estimated 1.1 million Pennsylvanians suffering from diabetes could benefit from a law enacted by the Pennsylvania General Assembly and signed by Governor Thomas J. Ridge in October of 1998. This new law mandates that private and group health insurance plans cover the costs of insulin, syringes, blood glucose monitors, testing strips and other supplies designed to help diabetics keep their disease in check. It also requires coverage for doctor-prescribed counseling that helps patients stick with their diet and other necessary life-styles changes.
The Pennsylvania Health Care Cost Containment Council supported this legislation, with the exception of a provision to cover hearing aids, by virtue of a mandated benefit review. Under the Council's enabling legislation, Act 89 of 1986 (as reauthorized by Act 34 of 1993) the Council is charged with reviewing existing or proposed mandated health benefits when requested by the executive and legislative branches of government. The Council found that while mandated insurance coverage for these diabetes-related benefits may initially cost between $171 million and $256 million a year, the long term savings in diabetes treatment costs can reach billions of dollars.
This report begins a process of tracking the impact of the new law on the cost and quality of treatment for diabetes.
While there is no cure for diabetes, the impact of it can be treated and controlled through medication, diet and other life-styles changes. In many ways, therefore, a hospitalization for diabetes or a diabetes-related complication may represent a failure of the primary care system. Patients may be improperly diagnosed and treated, and patients may fail to follow the treatment regimen. Consequently, their condition worsens and eventually hospitalization is necessary. That is why this report, and others to follow, focuses on the number of hospital admissions for diabetes and diabetes-related complications such as eye and heart diseases. By monitoring initial and repeated hospital admissions, hospital charges, and lengths of hospitalization, policy makers can, over time, observe whether this new mandated benefit is, in fact, having the desired effect. A focus on improved treatment of diabetes should, theoretically, result in fewer admissions and readmissions, particularly for the treatment of short-term complications stemming from diabetes.
In addition, a focus on diabetes represents an opportunity to further report payor-related data. Vast changes in the health care delivery system make it necessary to examine the interrelationships of care. This is especially the case when dealing with a chronic disease where preventing hospitalizations is possible. Managed health care insurance plans in particular have marketed themselves based, in part, on an emphasis in preventive and primary care; a part of "managing care." Focusing on statistics such as diabetes-related hospitalizations over time presents an opportunity to observe whether such efforts by managed care plans and other providers are having an impact. The Council plans to focus on this subject in a future report.
Diabetes is a chronic disease that has no cure. Nearly 16 million people in the United States have diabetes, 5.9% of the population. According to the Centers for Disease Control and Prevention, there are 10.3 million Americans with diagnosed diabetes and an additional 5.4 million Americans with undiagnosed diabetes.
Since 1983, the number of Americans with diabetes has increased by 50%. This increase is due to an aging, overweight and sedentary population. If this trend continues, diabetes and its complications will have an increasingly significant impact on the cost and quality of health care in this country.
Diabetes is the seventh leading cause of death in the United States. Diabetes was determined to be either the underlying or a contributing cause of death in approximately 12,000 Pennsylvania residents.
It is estimated that one third of all people with diabetes do not know they have it or do not discover it until they develop one of its life threatening complications such as heart or kidney disease.
Furthermore, people with diabetes lose more work time than their peers. According to the American Diabetes Association, diabetes costs Pennsylvanians an estimated $6.7 billion in medical costs and lost productivity each year.
According to the Council's database, diabetes-related inpatient hospitalizations accounted for 14.7% of all inpatient admissions during 1997. These 262,817 inpatient admissions resulted in approximately $4 billion in charges for hospital treatment and absorbed nearly 2 million hospital days.
Top Five Average Death Rates for Diabetes as any Listed Cause, by State
(per 100,000)--1992-1994
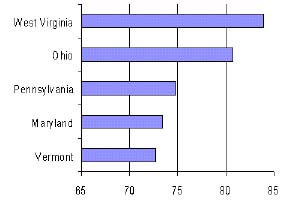
* Source: Centers for Disease Control and Prevention.
This report covers 1997 diabetes-related inpatient hospitalizations. Diabetes-related inpatient hospitalizations are defined as those inpatient hospitalizations coded with diabetes as the primary or secondary diagnosis. It is important to note that the study population includes patients who have diabetes but who were hospitalized for reasons unrelated to their diabetes - i.e., hip replacement. In those cases, diabetes is listed as a secondary diagnosis because it is important for the health care team to be aware of potential risks and complications that may develop due to the patient's diabetes.
Due to the coding system used by hospitals, the Pennsylvania Health Care Cost Containment Council is unable to distinguish type 1 diabetes in the hospital coding. Therefore, this report consists of diabetes-related inpatient hospitalizations and complications for Insulin Dependent Diabetes Mellitus (IDDM) and Non-Insulin Dependent Diabetes Mellitus (NIDDM) patients. For this report, IDDM is defined as any patient who needs daily injections of insulin to sustain their life regardless of whether they are clinically defined as having type l or type 2 diabetes. NIDDM is defined as any patient who controls their diabetes through diet and exercise, oral medication, or a combination of both.
Diabetes mellitus is a group of diseases characterized by high levels of blood glucose resulting from defects in insulin secretion, insulin action, or both. Insulin is a hormone that allows blood sugar to enter the cells and be used for energy. There are two principal types of diabetes:
Type 1 Diabetes (previously called juvenile-onset diabetes) - an autoimmune disease in which the body destroys the cells in the pancreas that produce insulin, typically resulting in a total failure to produce insulin. Without insulin the body cannot control blood levels of glucose. People with type 1 diabetes must take daily insulin injections to stay alive. Although type 1 diabetes usually appears in children or young adults, it may affect people at any age. According to the American Diabetes Association, the risk of developing type 1 diabetes is higher than virtually all other severe chronic diseases of childhood. Type 1 diabetes accounts for 5% to 10% of all diagnosed cases of diabetes.
Type 2 Diabetes (previously called adult-onset diabetes) - a metabolic disorder in which the body either produces insufficient amounts of insulin or does not have the ability to properly use the insulin it produces, resulting in a build up of sugar in the bloodstream. The Centers for Disease Control and Prevention estimate that 40 percent of people with type 2 diabetes require insulin injections. Other people with type 2 diabetes control their disease through oral medications, diet, and exercise. Type 2 diabetes is the most common form of diabetes and is estimated to account for about 90% to 95% of all diagnosed cases of diabetes. Type 2 diabetes typically occurs in people over age 45 who are overweight and sedentary.
A third type of diabetes, known as gestational diabetes, develops in 2% to 5% of all pregnancies but disappears when a pregnancy is over. However, nearly 40% of these women will develop type 2 diabetes later in life. Gestational diabetes occurs more frequently in African-Americans, Hispanic/Latino Americans, and American Indians.
Diabetes is a chronic disease that is estimated to affect more than 1 million Pennsylvanians. With 1 in 11 Pennsylvanians affected, the Commonwealth has one of the highest rates in the nation, accounting for 7% of the national total of 15.7 million cases.
According to National Centers for Disease Control data reported in an April 5, 1998 article in the Philadelphia Inquirer, the impact of diabetes has been particularly devastating in some rural areas. "Nine areas of Pennsylvania, covering 18 counties, had death rates that were double or triple the national rate for the period 1989-1992, federal data show."
The article notes that three of those areas, Tioga, Luzerne and Mercer Counties, "ranked among the 20 areas with the highest death rates nationally." The Council's data shows widespread variation in the number of diabetes-related inpatient hospitalizations across Pennsylvania counties. On the low side, Pike County had 9 (rounded up) residents per 1,000 hospitalized with diabetes. On the high side, Forest County had 44 (rounded up) residents per 1,000 hospitalized with diabetes.
Age
The prevalence of diabetes increases with age, a significant trend given the growing number of elderly Pennsylvanians.
The Pennsylvania State Data Center estimates that Pennsylvanians aged 65 years and older increased by 4.1% from 1990-1994. The largest increase occurred among those 85 and older (26.3%), compared to 1.5% growth rate for the state population as a whole.
Sex
In Pennsylvania, a higher proportion of women are hospitalized for diabetes-related causes. This is especially true between birth to 39 years of age and again after 60 years of age. This is also affected by the fact that women have a longer life expectancy than men.
Nationally, diabetes appears to affect men and women with equal frequency. According to the National Centers for Disease Control and Prevention, 8.2% of both men and women have diabetes.
Race/Ethnicity
The incidence of diabetes is affected by race/ethnicity. National figures indicate that non-Hispanic African Americans are 1.7 times as likely to have diabetes as non-Hispanic whites of similar age. Furthermore, on average, Hispanic/Latino Americans nationally are almost two times as likely to have diabetes as non-Hispanic whites of similar age.
Healthy People 2000, a national public health project of the federal Department of Health and Human Services, sets national goals for disease prevention and control. One objective is to reduce the prevalence rate of diabetes and its chronic disabling conditions among all adults to no more than 25 per 1,000. Although the rate is projected to decrease in Pennsylvania, the Pennsylvania Assessment Mid-Decade Review published by the Pennsylvania Department of Health in May, 1997, noted that, "the projected decreases will probably not be nearly enough to help Pennsylvania meet this national year 2000 objective."
The following table outlines the Healthy People 2000 goals, the Mid-Decade Review (1995) figures published by the Pennsylvania Department of Health, and the Department of Health projections for Pennsylvania by the year 2000.
| Subject | Goal for Healthy People 2000 | Pennsylvania's Actual Figures in 1995 | Pennsylvania's Projection for 2000 |
| Prevalence of Diabetes | 25 per 1,000 | 56 per 1,000 | 46-48 per 1,000 |
| Prevalence of Diabetes among African Americans | 32 per 1,000 | 72 per 1,000 | Unable to determine |
| Diabetes Death Rate | 34 per 100,000 | 45.5 per 100,000 | 45 per 100,000 |
| Diabetes Death Rate among African Americans | 58 per 100,000 | 71.3 per 100,000 | Unable to determine |
| Percentage of population who are over weight (weight is a contributing factor to diabetes) | 20% of population aged20 or older | 31% of population aged20 and older | 35% of population aged20 and older |
Eye Disease - Diabetes is the leading cause of new blindness in adults 20 to 74 years old. Every year there are 937 new cases of diabetes-related blindness in Pennsylvania. Additionally, people with diabetes are 60% more likely to develop cataracts and 40% more likely to suffer from glaucoma.
Kidney Disease - Diabetes is the leading cause of end-stage renal disease (kidney failure), accounting for 40% of new cases. Kidney disease is a significant cause of premature mortality in people with diabetes. In Pennsylvania, over 1,000 new cases of end-stage renal disease related to diabetes are diagnosed each year. The American Diabetes Association estimates that 50% of diabetes-related end-stage renal disease is preventable by controlling blood pressure.
Heart Disease - Adults with diabetes have heart disease rates two to four times higher than those without diabetes, Heart disease is the leading cause of diabetes-related deaths. The American Diabetes Association suggests that controlling blood pressure and lipids (such as cholesterol) combined with smoking cessation may prevent 45% of diabetes-related cases of heart disease.
Neurological Disease - About 60% to 70% of people with diabetes experience mild to severe forms of nervous system damage, known as diabetic neuropathy. This nerve damage can affect all areas of the body but is most common in the legs, feet, and hands. Severe forms of diabetic nerve disease are a major contributing cause of lower extremity amputations. Regular checkups and self-examination on a daily basis are recommended for people with diabetes. Tight control of blood glucose has shown to decrease the risk of developing neuropathy by as much as 69% among individuals with no existing conditions.
Vascular Disease - About 10% of people with diabetes have peripheral vascular disease which is reduced blood flow to the feet and legs. If left untreated this can lead to gangrene and amputation. Vascular disease is four times more common in people with diabetes. According to the American Diabetes Association, controlling blood pressure and smoking cessation can prevent 60% of diabetes-related vascular disease.
Amputation - More than half of lower extremity amputations in the United States occur among people with diabetes. The risk of leg amputation is 15-40 times greater for a person with diabetes. In Pennsylvania, over 5,100 cases involved lower extremity amputations or complications from previous amputations in 1997. The American Diabetes Association estimates that half of diabetes-related amputations can be prevented through improved glycemic control, education, improved control of blood pressure, and smoking cessation.
Stroke - The risk of stroke is two to four times greater in people with diabetes. Hypertension is more common in people with diabetes and a leading contributor to stroke and heart disease. An estimated 60% to 65% of people with diabetes have high blood pressure.
Ketoacidosis - Ketoacidosis is responsible for about ten percent of diabetes-related deaths in individuals under age 45 according to the American Diabetes Association. High blood glucose levels along with ketones in the urine mark diabetic ketoacidosis. This is one of the most serious outcomes of poorly controlled diabetes, and occurs primarily in type 1 individuals.
The causes of diabetes are not well understood, although both genetic and environmental factors such as obesity and lack of exercise appear to play roles.
Type 1 Diabetes - According to the American Diabetes Association, siblings of people with type 1 diabetes and children of parents with type 1 diabetes have an increased risk of developing the disease. Other factors such as illness also come into play for diabetes to develop. The Centers for Disease Control and Prevention states that autoimmune, genetic, and environmental factors are also involved in the development of type 1 diabetes. The risk factors are not well defined.
Type 2 Diabetes - The risk factors include people over age 45, obesity, physical inactivity, and family history of diabetes. Women with a prior history of gestational diabetes are also at increased risk for type 2 diabetes. African-Americans and Hispanic Americans are twice as likely to develop diabetes than the general population.
The symptoms of diabetes can develop gradually and are therefore frequently ignored. It is common for people to confuse the symptoms of diabetes as a sign of aging or the flu. Often people with diabetes have no symptoms at all.
Symptoms of Type 1 Diabetes:
Symptoms of Type 2 Diabetes:
A health professional should be consulted if one experiences any combination of these symptoms. Currently, the routine diagnostic test for diabetes is a fasting plasma glucose test that measures the level of glucose in the blood. A fasting plasma glucose value of greater than or equal to 126 milligrams/deciliter (mg/dl) indicates a diagnosis of diabetes.
Appropriate treatment can control blood sugar levels and help prevent or delay diabetes-related complications. Treatment involves proper nutrition, exercise and medication. According to the Centers for Disease Control and Prevention, training in self-management is integral to the treatment of diabetes.
Lack of insulin production by the pancreas makes type 1 diabetes particularly difficult to control. Treatment requires a strict regimen that typically includes a carefully calculated diet, exercise, home blood glucose testing several times a day, and multiple daily insulin injections. At this time, it is not possible to "take a pill" to provide the body with insulin since stomach acids would destroy the insulin before it could begin to work. Research into new treatment methods, including insulin delivery, is ongoing.
Treatment of type 2 diabetes typically includes diet control, exercise, home blood glucose testing, and in some cases, oral medication and/or insulin. Approximately 40% of people with type 2 diabetes require insulin injections.
Diabetes is a chronic disease associated with serious complications and premature death. The heavy financial and social burden of diabetes affects Pennsylvanians through high medical costs, lost work productivity and reduced quality of life. Through early detection and proper treatment, people can learn to control their diabetes and delay or prevent complications. Education and self-management are essential to the prevention of acute complications. Advances in technology, new treatments, and a transforming health care system give people with diabetes the incentives to be proactive in their care and, therefore, have a better quality of life.
American Diabetes Association Call
1-800-DIABETES
http://www.diabetes.org
Division of Health Statistics
Pennsylvania Department of Health
555 Walnut Street, 6th Floor Harrisburg, PA 17101-1900
Telephone: 717-783-2548 Fax: 717-772-3258
http://www.health.state.pa.us/hpa/stats/
Juvenile Diabetes Foundation
Call 1-800-223-1138
http://www.jdrf.org
 Facebook
Facebook